
TB Mukt Bharat: Challenges, Opportunities, and the Road Ahead

Abstract
Introduction
Tuberculosis (TB) is a preventable and usually curable disease. However, it remains one of the world’s deadliest infectious diseases, with over 10 million people falling ill and more than 1 million deaths annually worldwide, making it the leading cause of death from a single infectious agent and among the top 10 causes of death globally. Without treatment, the death rate from TB disease is high, with untreated smear-positive cases having a 10-year fatality rate averaging around 70%.[1] With WHO-recommended treatment regimens, typically 4–6 months of anti-TB drugs, about 90% of people with TB can be cured.
Global scenario:
Globally, TB incidence was estimated at 131 cases per 100,000 population in 2024. Among the 30 high TB burden countries, most have improved service coverage between 2000 and 2019, with the largest absolute gains seen in China, India, Myanmar, Thailand, and Vietnam. In India, TB incidence declined from 237 per lakh to 187 per lakh population, while mortality decreased from 28 to 21 per lakh from 2015 to 2024. All WHO and UN Member States have committed to ending the global TB epidemic through the End TB Strategy and Sustainable Development Goals (SDGs). The 2030 targets of the End TB Strategy aim for a 90% reduction in TB deaths and an 80% reduction in TB incidence compared to 2015 levels, with interim 2025 milestones of 75% and 50% reductions, respectively. Despite significant progress, TB remains a major global public health challenge, with many regions falling short of these targets. The COVID-19 pandemic caused setbacks, but recent data show most indicators are improving, with notable regional and country successes.
Key updates under TB Mukt Bharat Abhiyaan:
India is making significant strides toward tuberculosis elimination, in terms of reduction in mortality (21 per lakh) and incidence (187 per lakh) by 28% to 21%, respectively. India diagnosed 2.61 million of the estimated 2.7 million TB cases in 2024, significantly closing the notification gap and missing cases (from 15 lakhs to < 1 lakh) from baseline to 2024. Further and faster reductions in TB burden as per the set target of achieving mortality 3 per lakh and incidence 47 per lakh require enhanced coverage of diagnostic, treatment, and preventive services; addressing social determinants that fuel new infections and disease progression; and breakthroughs such as new TB vaccines.[2] State-Level Performance: Achievers: States like Kerala excel for significant drops in TB incidence (83 per lakh) and mortality (14 per lakh) due to a combination of decentralised governance, aggressive technology adoption, active private-sector alignment, leveraging strong private sector engagement, nutrition support, and digital monitoring. Their success is driven by treating TB elimination as a social movement rather than just a medical campaign.
State-Level Strugglers:
While some states have made tremendous progress, however, several states like Uttar Pradesh, Bihar, Madhya Pradesh, Jharkhand, and Rajasthan- are struggling with the TB burden. According to national data, Uttar Pradesh alone accounts for approximately 20% of India’s drug-sensitive TB cases.[3] These states face challenges including human resource shortages, persistent stigma, and weak integration with other health programs, hindering progress.
Key challenges:
Despite
this, there is a long way to go to achieve a significant reduction in high
incidence and prevalence of TB in India. Factors like lack of awareness and
resources, poor infrastructure, increasing drug-resistant cases, poor
notification and overall negligence are the major challenges. If we eradicate
poverty and undernourishment, educate the masses and eliminate the stigma
attached to TB, we can hope for a disease-free future.[4] The social
conditions and co-morbidities that fuel the TB epidemic have been very poorly
addressed in India. An estimated 300 million Indians still live in extreme
poverty. India has been called the ‘epicentre of global malnutrition and the
high prevalence of malnutrition is well documented.[5] Diabetes is
another important risk factor for TB.[6] Furthermore, tobacco
smoking is strongly associated with a higher risk of TB mortality; according to
one estimate, smokers accounted for 66% of males who died from TB in India.[7]
Analytical Tools:
SWOT Analysis: A comprehensive SWOT analysis can navigate the complexities of tuberculosis control in India.[8] By leveraging strong political will, advanced diagnostics, and digital tools, the program shall address critical challenges such as private sector engagement gaps, workforce limitations, and social stigma. Coupled with opportunities from global partnerships and health initiatives like Ayushman Bharat, NTEP strategically confronts threats including drug-resistant TB and resource constraints, ensuring a focused and adaptive approach to eliminating tuberculosis nationwide. (Table 1)
STRENGTHS | Weaknesses (Internal Negative) | OPPORTUNITIES | THREATS |
|---|---|---|---|
· Human & Institutional Resources: Committed frontline, clinical, and laboratory staff · State Task Force: Active Medical College and State-level bodies for regular clinical review and strict monitoring · Physical Infrastructure: Standardized Operational Procedures (SOPs) implemented nationwide. | · Clinical & Diagnostic Challenges · Complex TB Forms: Growing burden of Drug-Resistant TB (DR-TB) and Extrapulmonary TB (EPTB). · Vulnerable Demographics: High difficulty in accurate Paediatric TB diagnosis due to low-bacterial load samples. · Diagnostic Gaps: Shortages or uneven distribution of ultra-portable digital X-ray machines and logistics issues in patient/ sample transportation. | · High-Level Political Will: National commitment from leadership to achieve early elimination targets. · Uncapped Funding: Substantial external fiscal support from the World Bank, corporate CSR, and central/ state budgetary channels. | · Socio-Cultural Barriers · Social Stigma: Widespread fear of social isolation leading to patient concealment of symptoms and delayed care. · Religious & Cultural Beliefs: Alternative healing claims that pull patients away from evidence-based allopathic treatment. |
· Financial & Governance · Robust Funding Ecosystem: Strong internal fiscal pipeline via NTEP budgets, State TB Divisions, and the State Health Systems Resource Centre (SHSRC). · Good Governance: Strong administrative frameworks driving public health execution · Aggressive Active Case Finding: Time-bound, high-impact interventions like 100-day TB campaigns. · Advanced Diagnostic Network: Universal molecular testing using the Hub & Spoke model (CBNAAT/TrueNAT). | · Treatment Adherence: Challenges in maintaining long-term drug compliance across multi-month regimens. · Co-morbidities: Compounding health factors like severe malnutrition, HIV, and Diabetes. · Prevention Hurdles: Poor community or clinical acceptability of TB Preventive Treatment (TPT) among household contacts. · Private Sector Delays: Historically weak or uneven involvement of private practitioners leading to delayed or missing cases. · Data Disconnect: Under-reporting, under-notification, and gaps in generating continuous, long-term post-treatment follow-up reports. | · Public-Private Partnership (PPP) Models: Strategic engagement of corporate hospitals, local chemists, and private clinics to route patients into public care. · Nikshay Mitra Initiative: Community-driven adoption of TB patients by individuals, NGOs, and corporates for nutritional/vocational support. · Nikshay Poshan Yojana/ Poshan Abhiyan: Direct Benefit Transfer (DBT) monthly financial support to fight patient undernutrition. · Administrative Oversight: High-level administrative reviews (e.g., Additional Chief Secretary/ Senior Institutional Reviews) to clear bureaucratic bottlenecks. | · Migration & Urbanization: Highly mobile migrant populations (e.g., construction workers, daily labourers) leading to loss-to-follow-up and broken treatment cycles. · Persistent Malnutrition: Macro-economic food insecurity acting as a constant generator of new TB cases. |
· Core Processes & Interventions · Early Mitigation: Universal Drug Susceptibility Testing (UDST) for immediate drug-resistance detection. · Patient Care Models: The Differentiated Care Model to clinically risk-stratify patients at diagnosis. · Digital Monitoring & Compliance: Streamlined TB notifications and the 99DOTS / Nikshay 2.0 (99DOTS Lite) system for digital medication adherence. · Incentivization: Direct financial incentives for ASHA workers for successful patient tracking and treatment completion. | · Operational & Patient Gaps · Treatment Adherence: Challenges in maintaining long-term drug compliance across multi-month regimens. · Co-morbidities: Compounding health factors like severe malnutrition, HIV, and Diabetes. · Prevention Hurdles: Poor community or clinical acceptability of TB Preventive Treatment (TPT) among household contacts. · Private Sector Delays: Historically weak or uneven involvement of private practitioners leading to delayed or missing cases. | · Research Opportunities: Scope for indigenous vaccine development, shorter drug regimens, and artificial intelligence (AI) integrated digital chest X-ray screening. | · External Disruptions · Informal Providers (Quacks): Unregulated, non-certified local practitioners providing incorrect, incomplete, or irrational drug prescriptions |
· Evolving Frameworks: Regularly customized, data-driven national clinical guidelines based on past experiences (e.g., transition from traditional DOTS to daily regimens | · Data Disconnect: Under-reporting, under-notification, and gaps in generating continuous, long-term post-treatment follow-up reports. | · Research Opportunities: Scope for indigenous vaccine development, shorter drug regimens, and artificial intelligence (AI) integrated digital chest X-ray screening. | · Media Narrative: Negative or sensationalized media coverage regarding drug shortages or side effects, creating panic and eroding community trust in public health facilities. |
TOWS:
The TOWS Matrix is a strategic planning framework that builds on the SWOT analysis by matching internal strengths and weaknesses with external opportunities and threats, used to transition situational assessments (like SWOT) into actionable strategies. It matches internal strengths and weaknesses against external opportunities and threats to optimise TB eradication efforts.[9] (Table 2)
| Strategy Type | Focus | Description |
|---|---|---|
| SO (Maxi-Maxi) Strength–Opportunity | Aggressive/ Growth | Use internal strengths to maximize external opportunities. Use political commitment + digital tools to expand case detection |
| ST (Maxi-Mini) (Strength–Threat) | Competitive/ Defensive | Leverage internal strengths to minimize or avoid external threats. Leverage Ayushman Bharat to counter overcrowding risks |
| WO (Mini-Maxi) (Weakness–Opportunity | Developmental | Improve internal weaknesses by exploiting external opportunities. Address HR shortages via NGO partnerships |
| WT (Mini-Mini) | Retrenchment/ Survival | Minimize weaknesses and avoid external threats to survive. Strengthen governance to reduce funding delays |
Logical Framework Analysis (LFA):
Under the NTEP is a strategic planning and management tool. It provides a systematic, structured matrix to define project goals, activities, and expected results. This approach maps out how program inputs will achieve objectives and sets standards for Monitoring and Evaluation (M&E). Log Framework is a foundational system for recording and monitoring TB program activities, ensuring accurate data collection and timely reporting to evaluate performance and guide strategic decisions. This framework integrates diverse data sources (Ni-kshay, Lab registers, HMIS, TB Report) and focuses on indicators (Detect, Treat, Prevent, Build) supported by continuous monitoring and independent audits to ensure accountability and guide improvements.[10] (Table 3)
Level | Description | Indicators | Assumptions / Enablers |
|---|---|---|---|
Goal | Achieve TB-free India by 2027, reducing TB incidence and mortality in line with WHO End TB targets. | - TB incidence reduced by ≥80% (from 187 per lakh to <40 per lakh) - TB mortality reduced by ≥90% (from 21 per lakh to <2 per lakh) - ≥90% treatment success rate | - Sustained political commitment and funding - Cross-sector collaboration (health, housing, nutrition) - Continued innovation and community participation |
Outcome | Strengthened TB control system ensuring early detection, complete treatment, and prevention of transmission. | - ≥95% case notification through Ni-kshay - ≥90% adherence to treatment - ≥80% coverage of preventive therapy among contacts | - Private sector engagement maintained - Digital tools effectively scaled - Community trust and participation sustained |
Output | Improved service delivery and integration across health programs. | - ≥90% facilities using Ni-kshay portal - ≥80% HR trained in TB management - ≥70% districts certified TB-free - ≥90% beneficiaries receiving Nikshay Poshan support | - Timely fund release and HR deployment - Effective inter-program coordination - Stable supply chain for diagnostics and drugs |
Activities | 1. Strengthen case detection and notification 2. Enhance treatment adherence (digital tools, DOTS) 3. Train and retain HR in remote areas 4. Integrate TB with HIV, nutrition, and maternal health programs 5. Conduct IEC campaigns to reduce stigma 6. Expand Nikshay Poshan and transport support 7. Scale up MDR/XDR TB management (BPaLM regimen) 8. Improve living conditions and ventilation 9. Streamline funding and monitoring mechanisms | - Number of trainings conducted - IEC campaigns executed - Digital adherence tools deployed - MDR/XDR TB regimens scaled - Funding utilization rate ≥90% | - Coordination among ministries - Adequate logistics and technology support - Active participation of NGOs and Nikshay Mitras |
Stakeholder Matrix:
Map influence and interest. The Stakeholder Matrix maps key actors in NTEP by their level of influence and interest, clarifying their roles and contributions. This tool aids in prioritising engagement strategies to ensure effective collaboration and resource allocation for tuberculosis control.[11] (Table 4)
Stakeholder | Influence | Interest | Role/Contribution |
|---|---|---|---|
Government | High | High | Policy formulation, funding, oversight |
Healthcare Providers | High | High | Diagnosis, treatment, patient care |
NGOs | Medium | High | Community outreach, advocacy, support |
Patients | Low | High | Treatment adherence, feedback |
Private Sector | Medium | Medium | Notification, treatment, collaboration |
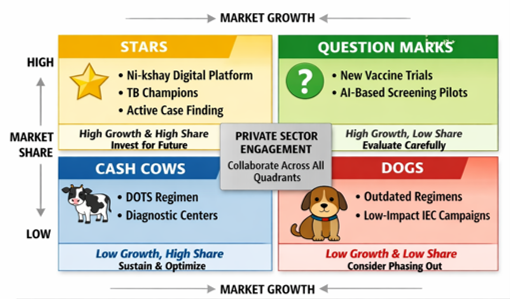
The BCG Matrix:
A strategic management tool developed by the Boston Consulting Group in the 1970s to help organisations analyse their portfolio of products or programs based on market growth and market share.[12] The BCG Matrix categorises interventions into Stars, Cash Cows, Question Marks, and Dogs, guiding resource allocation based on performance and growth potential to enable evidence-based prioritisation. For NTEP, this matrix serves as a strategic lens for decision-making within the National Strategic Framework, helping policymakers and program managers allocate resources based on performance and potential growth.[13] (Figure 1) TOWS and BCG Matrix are helpful to guide resource allocation.
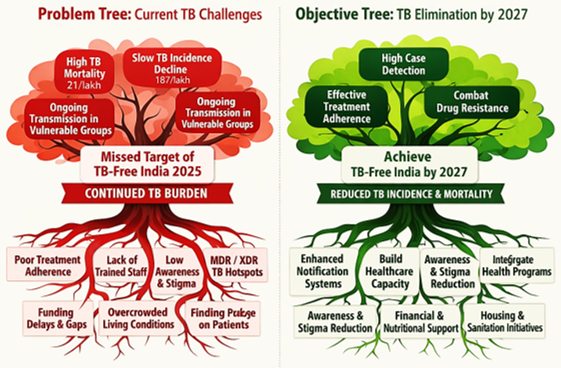
Problem Tree & Objective Tree:
These tools are vital visual tools in NTEP that help systematically identify and frame core problems, then translate them into clear, actionable goals.[14] By mapping root causes and their effects, the Problem Tree highlights key challenges, while the Objective Tree converts these into strategic objectives, guiding focused planning and effective implementation toward tuberculosis elimination. (Figure 2)
Evaluation Framework:
This framework integrates diverse data sources to comprehensively track program performance. It tracks the four national pillars (Detect, Treat, Prevent, Build) across four stages: Input, Process, Output, and Outcome. This ensures targets like early diagnosis and high cure rates are met.[15] (Table 5)
Stage | Focus | Key NTEP Indicators Measured |
|---|---|---|
Input | Resources needed for the program | Budget allocated, staff trained, testing machines (CBNAAT/TrueNat) available, and drug stocks |
Process | Day-to-day operations and activities | Turnaround times for test results, testing of household contacts, and timely initiation of treatment |
Output | Direct results of the program | Number of TB cases notified, percent of patients with known drug-sensitivity status, and people screened |
Outcome | Long-term impact on TB | Treatment success rates, reduction in death rates, and decrease in total TB cases (TB-Free target) |
Conclusion
India’s steady decline in TB incidence underscores the impact of sustained commitment, community participation, and robust public health initiatives; strong public health initiatives truly make a difference. With continued vigilance, expanded access to care, and collective responsibility, the country is moving closer to a future where TB-free India is not just a goal, but an achievable reality. Continued vigilance, expanded care access, and collective responsibility are key to achieving a TB-free India. India has made historic strides, yet elimination as per the target set requires shifting from basic clinical control to deep health system and social transformation. The remaining gaps demand an aggressive, localised, and multi-sector approach to finally end the epidemic.
References
- Tiemersma EW, van der Werf MJ, Borgdorff MW, Williams BG, Nagelkerke NJ. Natural history of tuberculosis: duration and fatality of untreated pulmonary tuberculosis in HIV negative patients: a systematic review. PLoS One. 2011 Apr 4;6(4):e17601. doi:10.1371/journal.pone.0017601. PMID: 21483732; PMCID: PMC3070694.
- Global tuberculosis report 2025. Geneva: World Health Organization; 2025.
- Kerala tops Niti Aayog’s health performance rankings, UP at bottom. The Times of India [Internet]. 2021 Dec 27. Available from: https://timesofindia.indiatimes.com/india/kerala-best-state-on-health-parameters-up-worst-niti-aayog-index/articleshow/88519727.cms
- Thakur G, Thakur S, Thakur H. Status and challenges for tuberculosis control in India - Stakeholders' perspective. Indian J Tuberc. 2021 Jul;68(3):334-339. doi:10.1016/j.ijtb.2020.10.001. Epub 2020 Oct 12. PMID: 34099198; PMCID: PMC7550054.
- Bhargava, Anurag & Sharma, Andrea & Oxlade, Olivia & Menzies, Dick & Pai, Madhukar. (2014). Undernutrition and the incidence of tuberculosis in India: National and subnational estimates of the population-attributable fraction related to undernutrition. The National Medical Journal of India. 27. 128-133.
- Harries AD, Lin Y, Satyanarayana S, Lönnroth K, Li L, Wilson N, Chauhan LS, Zachariah R, Baker MA, Jeon CY, Murray MB, Maher D, Bygbjerg IC, Enarson DA, Billo NE, Kapur A. The looming epidemic of diabetes-associated tuberculosis: learning lessons from HIV-associated tuberculosis. Int J Tuberc Lung Dis. 2011 Nov;15(11):1436-44, i. doi:10.5588/ijtld.11.0503. Epub 2011 Sep 6. PMID: 21902876.
- Jha P, Jacob B, Gajalakshmi V, Gupta PC, Dhingra N, Kumar R, Sinha DN, Dikshit RP, Parida DK, Kamadod R, Boreham J, Peto R; RGI-CGHR Investigators. A nationally representative case-control study of smoking and death in India. N Engl J Med. 2008 Mar 13;358(11):1137-47. doi:10.1056/NEJMsa0707719. Epub 2008 Feb 13. PMID: 18272886.
- Panigrahi S, Parida D, Sinha A, Sahoo KC, Bhattacharya D, Pati S. Integrated tuberculosis-multimorbidity management in India: A SWOT Analysis. Indian J Med Res. 2026;164:43-9. doi:10.25259/IJMR_2790_2025
- An Introduction to the TOWS matrix: Putting SWOT into action [Internet]. Professionalacademy.com. [cited 2026 July 8]. Available from: https://www.professionalacademy.com/blogs/an-introduction-to-the-tows-matrix-putting-swot-into-action/
- Central TB Division, Ministry of Health with Family Welfare, India. National strategic plan [NSP] for TB elimination 2017-25 [Internet]. 2017 Mar [cited 2026 July 9]. Available from: https://tbcindia.mohfw.gov.in/wp-content/uploads/2023/05/National-Strategic-Plan-2017-25.pdf
- Strategy for TB MUKT BHARAT ABHIYAAN - National TB Elimination Programme (NTEP) [Internet]. New Delhi: Central TB Division, Ministry of Health & Family Welfare; 2025. Available from: https://tbcindia.mohfw.gov.in/wp-content/uploads/2025/09/Guidance-Document-on-TB-Mukt-Bharat-Abhiyan_0.pdf
- Henderson B. The product portfolio [Internet]. BCG Global. 1970 [cited 2026 July 9]. Available from: https://www.bcg.com/publications/1970/strategy-the-product-portfolio
- Boston consulting group (BCG) Matrix [Internet]. Corporate Finance Institute. 2020 [cited 2026 July 9]. Available from: https://corporatefinanceinstitute.com/resources/management/boston-consulting-group-bcg-matrix/
- Problem analysis approaches. In: WASH and Health working together: a ‘how-to’ guide for neglected tropical disease programmes. Geneva: World Health Organization; 2018. p.167-172.
- India speeding towards TB elimination - PIB Backgrounder [Internet]. pib.gov.in. 2026 [cited 2026 July 9]. Available from: https://www.pib.gov.in/PressReleasePage.aspx?PRID=2244661®=3&lang=1