
Systematic Review
Association Between Anaemia and Handgrip Strength: A Systematic Review and Meta-Analysis
, Varsha Gadhavi  , Kripanshu Garasiya* ,
, Kripanshu Garasiya* ,
, Kripanshu Garasiya* ,
- 1 Indian Institute of Public Health, Gandhinagar, India

*Correspondence: Kripanshu Garasiya, kgarasiya@iiphg.org
Abstract
Introduction: Anaemia impairs oxygen delivery to tissues, potentially compromising muscle function. Handgrip strength (HGS) is validated marker of muscle function, frailty, and other health outcomes. Objective: To synthesize evidence on the association between anaemia and HGS in adults across diverse settings. Methods: MEDLINE, JSTOR, and Google Scholar were searched up to May-2025 using MeSH terms and keywords related to anaemia and handgrip strength. Of 510 identified records, 12 studies met the inclusion criteria. Two reviewers independently screened studies, extracted data, and assessed risk of bias using Joanna Briggs Institute checklists. Random-effects meta-analysis was performed in RevMan(v4.3.0) to pool odds ratios for weak handgrip strength among anaemic versus non-anaemic individuals. Results: Across studies, anaemia was consistently associated with poor HGS. Meta-analysis included three studies that provided comparable effect estimates and sufficient quantitative data for pooling; the remaining studies were synthesized narratively indicated that individuals with anaemia had 59% greater odds of weak grip strength (OR=1.59, 95%CI,1.07–2.37), with considerable heterogeneity. Subgroup analysis revealed stronger associations in men (OR=2.13, 95%CI,1.35–3.34) than in women (OR=1.30, 95%CI,1.05–1.78), and the effects were more pronounced in older adults (particularly in >65 years). Conclusion: Anaemia is associated with reduced handgrip strength, particularly among men and older adults in our findings. These findings suggest that handgrip strength may reflect functional impairment related to anaemia and could be useful as simple functional assessment measure in resource-limited settings. Further longitudinal studies are needed to clarify causality and the impact of anaemia treatment on muscle strength and functional outcomes.
Keywords: Anaemia, Hand Strength, Mass Screening
Introduction
Handgrip strength (HGS) is an objective and reproducible marker of muscular function and overall physical health. It is widely used as a surrogate indicator of sarcopenia and frailty and has prognostic value for cardiometabolic disease, disability, and mortality.[1] Another study conducted by Lee Wei et al.[2] reported that relative HGS could be used to assess cardiovascular health in public health. Similarly, a study among Canadian children and adolescents aged 6–19 years reported that HGS was associated with cardiometabolic health.[3] Another study reported an inverse relationship between HGS and mortality risk.[4] Another study reported that HGS was useful in the prediction of overall health outcomes.[5] Given the growing evidence linking muscle strength with overall health status, examining the association between anaemia and HGS may provide important insights into functional health and nutritional status.
Anaemia is defined as a reduced red blood cell count or haemoglobin concentration in the body below 13 g/dl in men and 12 g/dl in women, leading to impaired oxygen delivery to tissues. According to the World Health Organization, anaemia affects approximately 40% of children aged 6–59 months, 37% of pregnant women, and 30% of women aged 15–49 years globally, contributing significantly to functional impairment, fatigue, reduced physical capacity, and poor health outcomes.[6] Anaemia is linked to both short- and long-term morbidity, with women, children under five, and adolescents being particularly vulnerable.[7] Its pathophysiological effects stem from reduced oxygen-carrying capacity, leading to tissue hypoxia and diminished muscular performance.
The biological plausibility of an association between anaemia and reduced muscle strength has been well established by several individual studies.[8,9] Anaemia reduces oxygen delivery to muscle tissue, thereby impairing mitochondrial oxidative metabolism, limiting ATP generation, and resulting in muscle fatigue and weakness.[10] In Yu-mi Gi et al[11], 2020 study, anaemia was negatively associated with both absolute and relative HGS indices, with stronger associations observed in men than in women. Using data from the Korean National Health and Nutrition Examination Survey, the study found that individuals with weak HGS had higher odds of anaemia, particularly men and those aged 65 years or older. In an Indonesian elderly population, haemoglobin levels were positively correlated with HGS, and anaemia was significantly associated with weak HGS.. This association was more pronounced in males and those aged 80 years and above.[12] Other studies have investigated haemoglobin thresholds, iron status markers, and their relationships with HGS, but the results remain heterogeneous and context specific.
Despite this growing body of evidence, the literature remains fragmented, with heterogeneity in study design, population characteristics, definitions of anaemia, and methods of HGS measurement. There is currently no systematic review that comprehensively synthesizes these findings across diverse settings. Such a synthesis is essential to clarify the strength and consistency of this association and to determine whether HGS could be integrated into anaemia-related screening and risk stratification strategies, particularly among older adults and populations in resource-limited settings where advanced diagnostic facilities are not readily available.
Therefore, this systematic review aimed to critically evaluate and summarize the available evidence on the association between anaemia and handgrip strength in adult populations across different geographic and clinical contexts.
Methods
Protocol and Registration:
The protocol was prospectively registered on PROSPERO (CRD420251047729). The review was conducted as per the methodology described in the Cochrane Handbook for Systematic Reviews of Interventions and is reported as per the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines.[13]
Search strategy:
We conducted a comprehensive search of MEDLINE (via PubMed), JSTOR, and Google Scholar for studies published up to May 2025, using a structured combination of MeSH terms and free-text keywords. The search focused on terms related to anaemia (e.g., “Anaemia,” “Hemoglobin,” “Anemia”) and handgrip strength (e.g., “Grip Strength,” “Handgrip Strength,” “Dynamometer,” “Muscle Strength”). A PubMed search string included ‘("Anemia"[Mesh] OR anemia[tiab] OR hemoglobin[tiab]) AND ("Hand Strength"[Mesh] OR "Muscle Strength"[Mesh] OR "Grip Strength"[tiab] OR "Handgrip Strength"[tiab] OR "Hand Grip"[tiab] OR "Muscle Strength"[tiab] OR dynamometer[tiab] OR "hand-held dynamometer"[tiab])’. We also reviewed gray literature sources and the reference lists of key articles to identify additional studies. Only English-language published literature was included.
Eligibility criteria:
We included observational studies (cross-sectional, cohort, case‒control), interventional studies (RCTs or quasi experimental), or baseline data from trials reporting on the association between anaemia and handgrip strength in human populations of any age, sex, or setting (community-based or clinical). Anaemia had to be defined by objective haemoglobin measures (WHO or study-specific thresholds), and handgrip strength was measured quantitatively with validated dynamometry. Studies reporting comparative or association data between anaemia and HGS were needed. We excluded case reports, small case series (<10 participants), editorials, commentaries, letters, reviews, protocols, animal or in vitro studies, and any reports without quantitative data on anaemia or handgrip strength.
Study Selection:
Two independent reviewers screened the titles and abstracts retrieved from the search. Full-text articles were assessed for eligibility on the basis of the inclusion and exclusion criteria. Any disagreements between reviewers were resolved by discussion, and if needed, a third reviewer was consulted. The study selection process was documented via a PRISMA 2020 flow diagram, detailing the number of records identified, screened, excluded (with reasons), and included. All included articles were available in full text; therefore, no studies available only in abstract form were included in the review.
Data Extraction:
We developed and used a standardized data extraction form. Two reviewers independently extracted data on study characteristics (author, year, country, study design), participant demographics, sample size, definitions and measurements of anaemia and handgrip strength, effect estimates (e.g., mean differences, odds ratios), adjustment for confounding variables, funding sources, and conflicts of interest. Any discrepancies in data extraction were resolved through discussion.
Assessment of Risk of Bias:
The risk of bias for each included study was assessed independently by two reviewers via the Joanna Briggs Institute (JBI) critical appraisal checklists appropriate for the study design (e.g., cross-sectional, cohort, case‒control, RCT). (Supplementary File) The JBI critical appraisal tool includes structured questions to assess selection bias, measurement bias, confounding, and reporting bias. All judgments were documented, and disagreements were resolved through discussion or consultation with a third reviewer. We assessed the overall quality and certainty of evidence via established frameworks aligned with systematic review standards. Factors such as study design, risk of bias, consistency, directness, and precision were considered. Where applicable, subgroup analyses were planned by age group, sex, and health status to explore potential sources of heterogeneity and to improve the interpretability of pooled estimates. Each study was rated as having a low, moderate, or high risk of bias. Any disagreements were resolved by discussion or with input from a third reviewer.
Statistical analysis:
All the statistical analyses were conducted via R (version 4.3.0) with the meta package. In accordance with the registered protocol, a random-effects meta-analysis was performed where appropriate. Adjusted odds ratios (ORs) and 95% confidence intervals for the association between anaemia and weak handgrip strength were extracted. Heterogeneity was assessed via the I² statistic. Forest plots were used to visualize the effect estimates across studies. Owing to insufficient reporting across studies, planned subgroup and meta-regression analyses were not feasible.
Results
Study Selection:
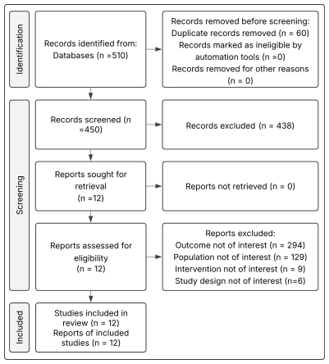
A total of 510 records were identified through electronic database searches. Following the removal of duplicates (n=60), 450 records were screened by title and abstract. Of these, 438 studies were excluded because they did not meet the eligibility criteria. The full texts of 12 studies were retrieved and assessed, all of which met the inclusion criteria. The study selection process is detailed in Figure 1.
Study characteristics:
The review included 12 studies with 50,045 participants and sample sizes ranging from 118 to 24,022. Studies were conducted in Australia, Indonesia, Korea, and Singapore (two each) and Brazil, Germany, Saudi Arabia, and the United States (one each). Seven studies were cross-sectional, one was a population-based cohort, three used secondary data, and one was cross-sectional longitudinal. Three studies involved 2,102 participants aged ≥65 years, six included 4,938 participants aged ≥60 years, and one in Australia included 640 women aged 18–49 years. A longitudinal study in Australia involved 1,705 men aged ≥70 years, whereas two Korean studies included 24,022 participants aged ≥30 years and 16,638 aged >19 years.
Handgrip strength measurement:
Handgrip strength (HGS) was consistently measured via validated dynamometers, although the specific devices used varied. The JAMAR hydraulic dynamometer was employed in three studies, whereas the Smedley spring-type dynamometer was used in the study by Sutandyo et al.[12] Four studies utilized a Takei A5401 digital dynamometer (Japan). One study used an electronic dynamometer (CAMRY EH101; Almari & Simbawa[13]), and another used SAEHAN SH5001 hydraulic device.[14] Two studies did not specify the make or model of the device used. Definitions of low handgrip strength vary across studies. The most commonly applied cutoff was <28 kg for men and <18 kg for women, as seen in the studies by Sutandyo et al.[12], C.-T. Lee et al.[15], and Vanda Ho et al[16]. Lower thresholds were also reported, including <27 kg (men) and <16 kg (women) by Almari & Simbawa[13], <26 kg and <16 kg by Yu-mi Gi et al.[11], and <26 kg (men) by Hirani et al.[8] [Supplementary File 1, Table 1]
Table 1: Characteristics of the included studies
| Author, Year | Country | Study design | Objective of the study | Sample size | Participants included | Anaemia Definition and estimation method | Dynamometer with HGS threshold |
|---|---|---|---|---|---|---|---|
| Thein M et al., 2009 | USA | Cross sectional study | To evaluate the association of anaemia with health-related quality of life, functional status, depression, disability, and physical strength in older adults, independent of chronic disease. | 328 | ≥ 65 years | WHO standards (anaemia if Hb <13 g/dL in men and <12 g/dL in women | Handheld Dynamometer (in kg) |
| Hidayat G et al, 2011 | Indonesia | Cross-sectional study | To determine whether anaemia is a risk factor for reduced muscle strength, measured by handgrip strength, in elderly nursing home residents. | 118 | ≥60 years | Females: less than 12 gr/dl and males less than 13 gr/dl were categorized as anaemic | Dynamometer. |
| Hirani V et al, 2016 | Australia | Cross- sectional Longitudinal | To assess the associations between haemoglobin levels and sarcopenia, muscle strength, functional measures, and ADL/IADL disabilities in older Australian men. | 1705 | Men ≥ 70 years | Absorption spectrophotometry, used for Hb. WHO criteria (anaemia If Hb level < 13 g/dL | JAMAR Dynamometer (Promedics, Blackburn, UK). grip strength less than 26.0 kg versus grip strength 26.0 kg and more |
| Amaral C et al., 2020 | Brazil | Cross-sectional study on secondary data | To examine factors associated with low handgrip strength in older adults in Rio Branco, Acre, Brazil. | 1016 | ≥60 years | anaemia (haemoglobin ≤13 mg/dL in males, or ≤ 12 mg/dL in females) | SAEHAN SH5001 brand hydraulic hand Dynamometer |
| Yu-mi Gi et al, 2020 | Korea | Cross-sectional study | To examine the association between handgrip strength and anaemia in Korean adults using data from the 6th and 7th KNHANES, addressing previous inconsistencies in the literature. | 16,638 | > 19 years | The haemoglobin levels were measured using the cyanide-free sodium lauryl sulphate method. WHO standards (Anaemia if Hb <13 g/dL in men and <12 g/dL in women) | Digital grip strength dynamometer (TKK 5401; Takei Scientific Instruments Co, Ltd, Tokyo, Japan) was used 26 kg for men, 16 kg for women is considered |
| C.-T. LEE et al, 2021 | Singapore | Cross- sectional | To estimate the prevalence of anaemia in community-dwelling adults ≥65 years in Singapore and examine its association with cognitive function, physical function, and frailty. | 480 | ≥ 65 years | Automated haematology analyser used for HB, WHO standards (Anaemia if Hb <1 g/dL in men and <12 g/dL in women; Hb level of >10 g/dL for mild,7–10 g/dL for moderate, and <7 g/dl for severe | Dynamometers (Takei A5401, Japan) Low grip strength <28 kg for men and <18 kg for women |
| Vanda Ho, 2022 | Singapore | Cross sectional on secondary data | To examine the association of handgrip strength (HGS) with iron indices and inflammation. | 477 | ≥60 years | Not specified | hand dynamometers (Takei A5401, Japan) was used where Low muscle strength was defined as HGS < 28 kg for men and < 18 kg for women |
| Sutandyo N. et al, 2022 | Indonesia | Cross-sectional study | To determine the prevalence of anaemia and its association with handgrip strength in Indonesian older adults, addressing gaps in data on anaemia in Southeast Asia using a large, multiprovince sample. | 3192 | ≥60 years | HemoCue method used for HB estimation. WHO standards (Anaemia if Hb <13 g/dL in men and <12 g/dL in women) | Smedley Spring type dynamometer used Weak HGS = <28 kg for men and <18 kg for women |
| Lee B et al., 2023 | Korea | Cross-sectional study on secondary data | To assess the association of anaemia with absolute and relative hand grip strength (HGS) and evaluate whether relative HGS indices are useful as risk markers compared to other cost-effective methods. | 24,022 | ≥30 years | WHO standards (Anaemia if Hb <13 g/dL in men and <12 g/dL in women, less than 11.0 g/dL for pregnant women) | Digital grip strength dynamometer (T.K. K 5401, Japan) |
| Almari S & Simbawa M, 2024 | Saudi Arabia | Cross-sectional study | To examine the correlation between handgrip strength (HGS) and nutritional status, and to evaluate whether HGS can predict nutritional status in hospitalized older adults in Saudi Arabia. | 135 | ≥60 years | Not specified | Electronic handgrip dynamometer (CAMRY, Model 1 EH101) was used to measure HGS. low grip = <16 kg for women and < 27 kg for men |
| Hammer T. et al., 2024 | Germany | Cohort study | To analyse the association between haemoglobin and grip strength, accounting for ferritin as an indirect marker of iron storage, in community-dwelling older adults. | 1294 | ≥ 65 years | Photometry, 4.4–11.3 Giga/L. | JAMAR |
| MacLean B et al, 2024 | Australia | Cross Sectional study | To develop a non-invasive screening tool for iron deficiency in women aged 18–49 years and evaluate its acceptability in the community. | 640 | Woman of 18-49 age group | Hemocue Hb801 used for Hb estimation. Anaemia was defined as Hb < 120 g/L, a threshold of Hb < 130 g/L. ferritin <30 μg/L were classed as iron deficient | JAMAR Hydraulic Hand Dynamometer |
Haemoglobin estimation:
Haemoglobin was estimated via a variety of validated laboratory methods across the included studies. Hammer et al.[17] measured haemoglobin via photometry, reporting a reference range of 4.4–11.3 giga/L. Sutandyo et al.[12] and MacLean et al.[18] used HemoCue analysers, with the latter applying a threshold of <13 g/dL for defining anaemia. Among the twelve studies, eight adhered to the World Health Organization (WHO) criteria for defining anaemia, with cutoffs of <13 g/dL in men and <12 g/dL in women. The remaining studies employed either study-specific thresholds or additional biochemical markers, such as serum ferritin and transferrin saturation, to define anaemia status.
Association between Handgrip Strength and Anaemia:
Across individual studies, HGS consistently decreased with anaemia, although effect sizes and levels of statistical significance varied. Among the 328 older adults in the US studied by Stauder and Thein[19], participants with anaemia had significantly lower grip strength than did those without anaemia (21.3 vs. 24.1 kg, p=0.014) and reported greater fatigue, disability, and depressive symptoms. In an Indonesian study by Hidayat G et al.[20], mild anaemia in women was associated with weaker grip strength (β=3.17, p=0.008). In Hirani V et al.[8]’s study of Australian men aged 70 years and older, higher Hb levels were strongly associated with stronger grip strength, a reduced risk of sarcopenia, and better functional outcomes, with an adjusted β of 0.82 (95% CI 0.55–1.08) per g/dL increase. A Brazilian household survey of 1,016 older adults conducted by Amaral C et al.[14] revealed that anaemia conferred more than a fourfold increase in the odds of weak grip in men (aOR 4.15, 95% CI 2.09–8.21) and nearly a twofold increase in women (aOR 1.80, 95% CI 1.06–3.06), independent of body mass index and other covariates. In the large Korean KNHANES dataset (n=16,638), anaemia was associated with weak handgrip strength (OR 1.92, 95% CI 1.58–2.33), with a stronger effect in men (OR 2.13, 95% CI 1.35–3.34) and in participants aged 65 years or older (OR 1.92, 95% CI 1.42–2.58).[11] A Singaporean cohort of community-dwelling older adults (n=480) revealed that anaemia was significantly associated with frailty and lower grip strength; each 1 g/dL increase in haemoglobin was associated with a 6% reduction in the odds of frailty.[15] Another Singaporean study, the HOPE cohort (n=477), demonstrated that higher haemoglobin, ferritin, and transferrin saturation were independently associated with greater grip strength, whereas elevated hsCRP was inversely associated with greater grip strength.[16] An Indonesian multiprovince study of 3,192 older adults conducted by Sutandyo N. et al.[12] revealed a positive correlation between haemoglobin and grip strength (r=0.35, p<0.001) and an increased risk of weak grip strength in those with anaemia (OR 1.56, 95% CI 1.31–1.85), with the strongest associations among individuals aged 80 years and older. Lee BJ et al[10] reported that more than 24,000 Korean adults reported lower mean grip strength in anaemic participants than in their nonanemic counterparts, with adjusted odds ratios indicating a stronger effect in men than in women. A Saudi Arabian hospital-based study by Almari S & Simbawa M[13] of 135 participants revealed that low haemoglobin and malnutrition were independent predictors of reduced grip strength. A German cohort study (n=1,294) by Hammer T. et al.[14] demonstrated that the association between haemoglobin and grip strength was evident in women younger than 80 years and in men with ferritin concentrations ≥300 μg/L but absent in those over 80 years. MacLean B et al.[18] studied Australian reproductive-aged women (n=640) and confirmed that haemoglobin and ferritin levels were positively associated with grip strength, extending the relevance of this association to younger populations. The study-specific findings are presented in Table 2.
Table 2: Summary of Findings
| Author, Year | Participants | Outcome | Effect size | Other Key Findings |
|---|---|---|---|---|
| Thein M et al. (2009) | 328 | Anemic participants had lower HGS compared to nonanemic individuals (21.3 kg vs. 24.1 kg; p = 0.014). | 21.3 vs. 24.1 kg; P = 0.014 | Anemia was associated with low HGS, along with higher fatigue, depressive symptoms, and increased disability |
| Hidayat G et al (2011) | 118 | In women, mild anemia was linked to lower HGS in women | 12.36 kg vs. 14.68 kg; p = 0.027. B = 3.172, SE = 1.179, β = 0.230, p = 0.008 | Each 1 g/dL increase in hemoglobin was associated with a 3.1 kg increase in HGS; age, physical activity, and anemia were independent predictors of reduced HGS |
| Hirani V et al (2016) | 1705 | A consistent positive association between hemoglobin and grip strength was observed | β = 1.52, 95% CI: 1.27–1.78, age-adjusted (β = 1.05, 95% CI: 0.80–1.30), and multivariate-adjusted (β = 0.82, 95% CI: 0.55–1.08). | 1 gm increase in Hb was associated with reduced risk of sarcopenia, slow walking speed, poor HGS, activities of daily life, instrumental activities of daily life, and inability to stand from a chair. |
| Amaral C et al. (2020) | 1016 | Low HGS was associated with anemia in both men and women | Anemic men had more than fourfold increased odds of low HGS (aOR = 4.15; 95% CI: 2.09–8.21), and anemic women had nearly double the odds (aOR = 1.80; 95% CI: 1.06–3.06), compared to their nonanemic counterparts. | Low BMI and anemia were independently linked to reduced handgrip strength (HGS) in both sexes. Diabetes was associated with low HGS in men. Other factors in males were current or past smoking, poorer self-rated health, and dependence for daily activities. Among women, altered waist-to-hip ratio, insomnia, and physical activity related to commuting or work were also associated with low HGS. |
| Yu-mi Gi et al (2020) | 16,638 | Anemia was associated with weak HGS, particularly in men and older adults | Anemia occurs in the weak HGS group than the strong HGS group with OR = 1.92, 95% CI: 1.58–2.33 Association was greater for males (OR = 2.13, 95% CI: 1.35–3.34) and for those aged ≥65 years (OR = 1.92, 95% CI: 1.42–2.58). | High prevalence in participants with ≥65 years than below 65 years. Anemic Men reflected twice the odds of weak HGS |
| C.-T. LEE et al (2021) | 480 | Anemia was significantly associated with weak HGS and frailty | Hemoglobin levels and anemia were significantly associated with frailty (OR=2.28; 95% CI=1.02-5.10) odds after adjusting for potential covariates (OR = 0.94, 95% CI: 0.90-0.99). | Each 1 g/dL increase in hemoglobin was associated with a 6% decrease in frailty |
| Vanda Ho et al. (2022) | 477 | Higher HGS was correlated with higher hemoglobin and iron indices | In univariate analysis revealed that HGS was significantly associated with higher Hb (β = 2.10 95%CI 1.67–2.53, p < 0.01 | High hand grip strength was also associated with high iron, ferritin, TSAT, and lower transferrin and TIBC. Ferritin, TSAT, and hsCRP were independent predictors of HGS in multivariate analysis. |
| Sutandyo N. et al (2022) | 3192 | Hb was positively correlated with HGS (r = 0.349, p < 0.001). Anemia increased the risk of weak grip (OR = 1.557), especially in those ≥80 years (p < 0.001). | OR: 1.557; 95% CI: 1.314-1.846; p value: <0.001 | Weak HSG was associated with age ≥80 (OR: 5.234), age 70–79 (OR: 3.152), low BMI (OR: 1.827), and hypertension (OR: 1.340) |
| Lee B et al. (2023) | 24,022 | Mean HGS was higher in nonanemic vs. anemic individuals 38.97 kg vs. 30.84 kg in men, and 22.64 kg vs. 21.85 kg in women—with a stronger association observed in men. | Adjusted OR of association of anemia and HGS in dominant hand in Men was 0.58 (0.51–0.66) < 0.001 (Age) 0.63 (0.55–0.72) < 0.001 (Other covariates) and in women 0.81 (0.76–0.86) < 0.001 (Age adjusted) 0.87 (0.81–0.93) < 0.001 (Other covariate adjusted) | The mean value of HGS was lower in anemic individuals. Relative HGS was associated with anemia. |
| Almari S & Simbawa M (July 2024) | 135 | Low hemoglobin was an independent predictor of weak HGS | Participants with low HGS had low hemoglobin levels (p < 0.001) | Participants with low HGS had low lymphocyte levels (p = 0.040), high creatinine levels (p = 0.004), high blood urea nitrogen levels (p = 0.007), high CRP levels (p = 0.007), high HbA1c levels (p = 0.029), and high vitamin B12 levels (p = 0.042). Also 16% were malnourished and 38.74% were at the risk of malnutrition with low HGS. |
| Hammer T. et al. (2024) | 1294 | Positive association between hemoglobin and HGS in women <80 years and in men <80 years with ferritin ≥300 µg/L. No association was found in those >80 years. | The average grip strength in the study population was 38.73 ± 9.35 kg for men and 23.99 ± 7.14 kg for women. In women <80 years, β 0.923[95% CI 0.196, 1.650], In Men < 80 years, the association was significant when ferritin was ≥ 300 μg/L, β 2.028 [95% CI0.910, 3.146] | In men with ferritin ≥ 300 μg/L 1 gm of HB was associated with 2.559 kg in HGS. Each 1 g/dL increase in Hb corresponded to a 0.923 kg gain in women and 2.028 kg in men. |
| MacLean B et al (2024) | 640 | HGS was positively linked to Hb (p = 0.004) and ferritin level (p = 0.005). | Adjusted R2 = 0.012, p = 0.004 | HGS demonstrated potential as a noninvasive marker of iron deficiency in women of reproductive age |
Quantitative Synthesis:
Three independent estimates were eligible for quantitative pooling because they provided comparable effect measures (odds ratios with corresponding confidence intervals or sufficient raw data) for the association between anaemia and weak handgrip strength. In the primary meta-analysis, the sex-specific strata from Amaral et al.[14] (2020) were combined using inverse-variance weighting to generate a single overall estimate. Together with estimates from Gi et al.[11] (2020) and Sutandyo et al.[12] (2022), the pooled analysis showed that anaemia was associated with increased odds of weak handgrip strength (OR 1.59, 95% CI 1.07–2.37). Between-study heterogeneity was considerable (I² = 88.0%; τ² = 0.1047; Q = 11.63, df=2). Importantly, all three study-level estimates showed a consistent direction of effect, indicating higher odds of weak grip strength among participants with anaemia (Figure 2). The remaining included studies were not pooled because they lacked sufficient quantitative data, used different outcome definitions or reporting formats, or did not provide effect estimates suitable for meta-analysis.
In a sensitivity analysis, the male and female strata from Amaral et al.[14] (2020) were retained as separate estimates, resulting in four pooled effects. The association remained robust and slightly stronger (OR 1.94, 95% CI 1.46–2.57). The heterogeneity decreased but remained substantial (I² = 71.1%; τ² = 0.0509; Q = 8.69, df = 3) (Figure 3). This demonstrates that the findings were not an artifact of combining sex-specific estimates and confirms the stability of the association across analytic choices.
![Association of anaemia with hand grip strength (pooled analysis of three studies including the combined overall effect of Amaral et al.[14])](https://jpchr.com/jpchr/article/download/e26061401/version/32/html/213/F02.png)
![Association between anaemia and weak handgrip strength: sensitivity analysis (Amaral et al.[14] men and women separated)](https://jpchr.com/jpchr/article/download/e26061401/version/32/html/214/F03.png)
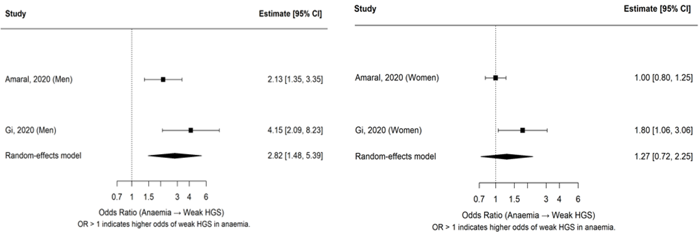
Subgroup analyses by sex were possible via data from Gi et al.[11] (2020) and Amaral et al.[14] (2020). Among men, anaemia was associated with markedly greater odds of weak grip strength (pooled OR 2.82, 95% CI 1.48–5.39), with moderate heterogeneity (I² = 60.6%; τ² = 0.1348; Q = 2.54, df = 1) (Figure 4a). In contrast, the pooled analysis for women suggested a weaker association (OR 1.27, 95% CI 0.72–2.25), accompanied by substantial heterogeneity (I² = 75.1%; τ² = 0.1297; Q = 4.01, df = 1) (Figure 4b). These divergent patterns suggest potential effect modification by sex, although the small number of available studies limits confidence in this interpretation. Assessment of small-study effects was not undertaken, in line with the Cochrane guidelines, given the inclusion of fewer than ten studies.
Taken together, the evidence from the available observational datasets consistently indicates that anaemia is associated with reduced muscle strength, measured objectively by handgrip strength testing. The primary and sensitivity analyses revealed higher odds of weak grip among individuals with anaemia, with the strongest and most consistent effects observed in men. Findings in women were less consistent and more heterogeneous. Studies incorporating biochemical indices of iron status (e.g., Ho et al.[16], 2022; Hammer et al.[17], 2024; MacLean et al.[18], 2024) further strengthen biological plausibility, showing positive associations of ferritin and transferrin saturation with grip strength and inverse associations for CRP.
Although substantial heterogeneity existed across studies, it likely stemmed from real differences in populations, protocols, and definitions rather than random noise. The effect direction remained consistent, with no contrary findings, strongly supporting anaemia as an independent driver of reduced muscle strength most clearly in men. These results emphasize incorporating anaemia screening into sarcopenia and frailty prevention, alongside calls for standardized methods and longitudinal research on age and sex-specific mechanisms.
A formal GRADE certainty assessment was not conducted. As all included studies were observational (cross-sectional or cohort designs) and generally judged at serious risk of bias, the certainty of evidence for all outcomes would begin at “low” and be further downgraded for risk of bias, inconsistency, and imprecision. Accordingly, overall certainty was considered “very low,” and no GRADE evidence table was presented.
Table 3: Risk of bias (JBI)
| Study No. | First Author (Year) | Was the sample frame appropriate to address the target population? | Were study participants sampled in an appropriate way? | Was the sample size adequate? | Were the study subjects and the setting described in detail? | Was the data analysis conducted with sufficient coverage of the identified sample? | Were valid methods used for the identification of the condition? | Was the condition measured in a standard, reliable way for all participants? | Was there appropriate statistical analysis? | Was the response rate adequate, and if not, was the low response rate managed appropriately? | Overall Appraisal | Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Alamri (2024) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Include | Appropriate sampling, valid measures, but response rate not reported. |
| 2 | Sutandyo (2022) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include | Very large national dataset with robust methodology. |
| 3 | Lee B (2023) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Include | Large sample, consistent tools, strong statistical analysis. |
| 4 | Hammer (2022) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Include | Response rate was 20% but data are available of 1294 |
| 5 | Hidayat (2011) | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | include | Valid measurement tools, but small sample size (~118). |
| 7 | Gi yu (2020) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include | Survey based study |
| 8 | MacLean (2025) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include | Well-designed, high response rate, solid methodology. |
| 9 | Lee C.-T. (2021) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include | Well-designed, high response rate, solid methodology. |
| 10 | Vanda ho (2022) | Yes | No | No | Yes | unclear | Yes | Yes | Yes | unclear | Exclude | No randomization in the sampling of participants, no evidence on the sample size calculation, no evidence on the response rate |
| 11 | Amaral (2020) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include | structured methodology and concrete statistical analysis |
| 12 | Thein (2010) | Yes | Unclear | Unclear | Yes | Unclear | Yes | Yes | Unclear | Unclear | Exclude | No evidence on randomization of participants, sample size calculation and response rate, unstructured methodology |
Discussion
A consistent association between anaemia and reduced handgrip strength (HGS) was observed across the included observational studies involving more than 50,000 participants. Individuals with anaemia generally demonstrated lower HGS compared to non-anaemic participants. The meta-analysis of three studies indicated increased odds of weak HGS among participants with anaemia. Several studies, including those by Stauder & Thein[19], Hidayat et al.[20], and Amaral et al.[14], also reported associations between anaemia and fatigue, disability, and poorer functional status, particularly in older adults. Although some studies suggested stronger associations in men and older age groups, these findings should be interpreted cautiously because subgroup observations were derived from a limited number of studies and substantial heterogeneity was present across study populations and methodologies.
In addition to demographic and lifestyle factors, several blood biomarkers were significantly associated with HGS. Biochemical markers, such as elevated CRP, reduced lymphocyte count, and increased blood urea nitrogen, creatinine, and HbA1c, are associated with reduced muscle strength. Longitudinal data from the CHAMP cohort revealed that higher haemoglobin levels predict stronger HGS and better physical function.[21] This relationship extends to younger populations, as seen in reproductive-age women, indicating anaemia’s impact across the life course. Iron profile parameters, particularly ferritin and transferrin saturation (TSAT), have been reported as associative factors.[16-18]
The biological plausibility of these associations is supported by the pathophysiology of anaemia. Reduced haemoglobin levels impair the oxygen-carrying capacity of blood, thereby limiting oxygen delivery to muscles and compromising their functional performance. This mechanism explains the frequent observation of reduced physical performance in anaemic individuals, including slower walking speed, increased fatigue, and a greater prevalence of depressive symptoms.[19]
Anaemia also becomes more prevalent with advancing age, particularly among older adults. In line with this, nine of the twelve included studies specifically recruited participants aged 60 years and above.[19] Frailty, another age-related condition, is common in this population and may act as a potential confounding factor in the association between anaemia and HGS.[21] Evidence from studies on red cell distribution width (RDW), a marker of erythrocyte size variation, further supports this complexity. A higher RDW was associated with lower grip strength, particularly in older men, and this relationship persisted even among nonanemic individuals.[22] These findings suggest that factors other than anaemia may contribute to reduced muscle strength. In addition, many studies have attempted to establish the association between low hand grip strength and mortality risk.[23–25] On the other hand, a low hand grip strength association was established with metabolic health in children and adolescents. Moreover, studies have shown that low hand grip strength is associated with increased hospitalization and quality of life.[22]
Heterogeneity in HGS assessment tools, such as the JAMAR and Takei A5401 dynamometers, along with varying HGS thresholds and anaemia definitions, has contributed to substantial variability across studies. The observational design introduced risks of bias and confounding, with associations weakening in the oldest-old individuals or varying with iron status. The lack of a universal HGS cutoff complicates interpretation, as it varies by demographic and clinical factors. Future research is warranted to address the comparability of data obtained via different assessment tools.
Longitudinal studies are needed to establish temporality, whereas interventional trials should test whether correcting anaemia improves HGS and related outcomes. Mechanistic studies could clarify the roles of haemoglobin, iron availability, and inflammation. Standardizing HGS measurement tools and thresholds would enhance comparability. Integrated screening strategies combining HGS with haematological testing could improve clinical and public health surveillance. Further exploration of the links between low HGS and metabolic health in younger populations and hospitalization risk could broaden the health implications of HGS.
Conclusion
In conclusion, anaemia’s strong link to reduced HGS highlights its role as a modifiable risk factor for muscle dysfunction, frailty, and poor quality of life across different populations. Integrating HGS as a simple, low-cost, non-invasive screening tool can improve anaemia detection and management. HGS may serve as a simple functional assessment measure associated with anaemia and reduced muscle strength. Given its ease of use and low cost, it could support functional health assessment in community and primary healthcare settings, particularly in resource-limited populations. Further longitudinal and interventional studies at different age group are needed to better understand its clinical utility and relationship with anaemia-related outcomes.
Given the observed association between anaemia and reduced handgrip strength (HGS), HGS may serve as a simple and non-invasive functional assessment tool in community and primary healthcare settings. Its ease of use and minimal equipment requirements could support early identification of individuals at risk of poor functional and nutritional health, particularly in resource-limited settings. Standardizing HGS protocols could position India as a leader in cost-effective surveillance, easing chronic disease burdens in elderly and underserved groups through scalable, equitable early interventions.
Declarations
Funding: No funding was received for this research.
Conflict of Interest: No conflicts of interest are declared.
References
- Vaishya R, Misra A, Vaish A, Ursino N, D’Ambrosi R. Hand grip strength as a proposed new vital sign of health: a narrative review of evidences. J Health Popul Nutr 2024;43(1):7. doi:10.1186/S41043-024-00500-Y.
- Lee WJ, Peng LN, Chiou ST, Chen LK. Relative handgrip strength is a simple indicator of cardiometabolic risk among middle-aged and older people: A nationwide population-based study in Taiwan. PLoS One 2016;11(8). doi:10.1371/JOURNAL.PONE.0160876.
- Rioux B V., Kuwornu P, Sharma A, Tremblay MS, McGavock JM, Sénéchal M. Association between Handgrip Muscle Strength and Cardiometabolic z-Score in Children 6 to 19 Years of Age: Results from the Canadian Health Measures Survey. Metab Syndr Relat Disord 2017;15(7):379–84. doi:10.1089/MET.2016.0147.
- López-Bueno R, Andersen LL, Koyanagi A, Núñez-Cortés R, Calatayud J, Casaña J, et al. Thresholds of handgrip strength for all-cause, cancer, and cardiovascular mortality: A systematic review with dose-response meta-analysis. Ageing Res Rev 2022;82:101778. doi:10.1016/J.ARR.2022.101778.
- Celis-Morales CA, Welsh P, Lyall DM, Steell L, Petermann F, Anderson J, et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: prospective cohort study of half a million UK Biobank participants. BMJ 2018;361. doi:10.1136/BMJ.K1651.
- Anaemia in women and children n.d.; https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children (accessed January 27, 2025).
- World Health Organization, Williams a L, van Drongelen W, Lasky RE, Sanderson M, Lai D, et al. Guideline : Daily iron and folic acid supplementation in pregnant women. World Health Organization 2012;46:323–9.
- Hirani V, Naganathan V, Blyth F, Le Couteur DG, Seibel MJ, Waite LM, et al. Low hemoglobin concentrations are associated with sarcopenia, physical performance, and disability in older australian men in cross-sectional and longitudinal analysis: The concord health and ageing in men project. Journals of Gerontology - Series A Biological Sciences and Medical Sciences 2016;71(12):1667–75. doi:10.1093/GERONA/GLW055.
- Penninx BWJH, Pahor M, Cesari M, Corsi AM, Woodman RC, Bandinelli S, et al. Anemia Is Associated with Disability and Decreased Physical Performance and Muscle Strength in the Elderly. J Am Geriatr Soc 2004;52(5):719–24. doi:10.1111/J.1532-5415.2004.52208.X.
- Lee BJ, Chi JH. Association between anemia and grip strength indices combined with anthropometry in the Korean population. Sci Rep 2023;13(1):18517. doi:10.1038/S41598-023-45985-5.
- Gi YM, Jung B, Kim KW, Cho JH, Ha IH. Low handgrip strength is closely associated with anemia among adults: A cross-sectional study using Korea National Health and Nutrition Examination Survey (KNHANES). PLoS One 2020;15(3). doi:10.1371/JOURNAL.PONE.0218058.
- Sutandyo N, Rinaldi I, Sari NK, Winston K. Prevalence of Anemia and Factors Associated With Handgrip Strength in Indonesian Elderly Population. Cureus 2022;14(5). doi:10.7759/CUREUS.25290.
- Alamri SH, Simbawa MM. The clinical utility of handgrip strength as a malnutrition screening tool in hospitalized older adults: a cross-sectional study in Saudi Arabia. Front Med (Lausanne) 2024;11. doi:10.3389/fmed.2024.1436977.
- De Araújo Amaral C, Amaral TLMI, Monteiro GTR, De Vasconcellos MTL, Portela MC. Factors associated with low handgrip strength in older people: Data of the Study of Chronic Diseases (Edoc-I). BMC Public Health 2020;20(1). doi:10.1186/s12889-020-08504-z.
- Lee C-T, Chen MZ, Yip CYC, Yap ES, Lee SY, Merchant RA. Prevalence of Anemia and Its Association with Frailty, Physical Function and Cognition in Community-Dwelling Older Adults: Findings from the HOPE Study. J Nutr Health Aging 2021;25(5):679–87. doi:10.1007/s12603-021-1625-3.
- Ho V, Lee CT, Merchant RA. The “Iron Tale”- iron indices and handgrip strength in community-dwelling adults. Aging Clin Exp Res 2022;34(12):3025–32. doi:10.1007/s40520-022-02242-5.
- Hammer T, Braisch U, Rothenbacher D, Denkinger M, Dallmeier D. Relationship between hemoglobin and grip strength in older adults: the ActiFE study. Aging Clin Exp Res 2024;36(1):59. doi:10.1007/S40520-024-02698-7.
- MacLean B, Lim J, Fuller J, Wylie R, Joo JY, Al-Sharea A, et al. Community screening for iron deficiency in reproductive aged women: Lessons learnt from Australia. Vox Sang 2025;120(1):22–31. doi:10.1111/vox.13750.
- Stauder R, Thein SL. Anemia in the elderly: clinical implications and new therapeutic concepts. Haematologica 2014;99(7):1127. doi:10.3324/HAEMATOL.2014.109967.
- Hidayat G, Kurnianda J, Pramantara IDP. ANEMIA AS RISK FACTOR OF HANDGRIP STRENGTH DECREASED ON ELDERLYIN YOGYAKARTAPROVINCE’S PANTI WERDHA. Acta Interna: The Journal of Internal Medicine 2011;1(1):10–4. doi:10.22146/acta.
- Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in Older People. Lancet 2013;381(9868):752. doi:10.1016/S0140-6736(12)62167-9.
- Orces CH. The Association Between Red Cell Distribution Width and Grip Strength in Older Adults. Cureus 2022;14(12). doi:10.7759/CUREUS.33049.
- Scherbov S, Spitzer S, Steiber N. Thresholds for clinical practice that directly link handgrip strength to remaining years of life: estimates based on longitudinal observational data. BMJ Open 2022;12(7):e058489. doi:10.1136/BMJOPEN-2021-058489.
- Wu Y, Wang W, Liu T, Zhang D. Association of Grip Strength With Risk of All-Cause Mortality, Cardiovascular Diseases, and Cancer in Community-Dwelling Populations: A Meta-analysis of Prospective Cohort Studies. J Am Med Dir Assoc 2017;18(6):551.e17-551.e35.doi:10.1016/j.jamda.2017.03.011.
- Lera L, Albala C, Leyton B, Márquez C, Angel B, Saguez R, et al. Reference values of hand-grip dynamometry and the relationship between low strength and mortality in older Chileans. Clin Interv Aging 2018;13:317–24. doi:10.2147/CIA.S152946